
Returned Sight in Blind SARDS Dogs With Early Endocrine Immune Management
Posted on September 17th, 2014This article is designed for the frustrated SARDS owner, who has had SARDS (Sudden Acquired Retinal Degeneration Syndrome) confirmed with an ERG and told there is no treatment for SARDS, and to go home and learn to live with a blind dog.
This seems to be the general veterinary belief regarding treating SARDS patients, that there is no cause and no treatment. But the truth is, there is a cause and a reason why SARDS develops, and there is a test and protocol to help treat SARDS patients that works!
The development of this syndrome is thought to come from an autoimmune disease in affected canine patients that destroys their retinal tissue. I have found, with my own clinical studies, each SARDS patient has an identifiable, endocrine immune imbalance that causes the immune cells of their body to be deregulated by a hormonal imbalance. This causes these immune cells to lose recognition of retinal tissue and attack the retinal tissue, as a foreign tissue.
This imbalance is easily identified and needs to be corrected as quickly as possible, in order to help avoid permanent, retinal damage. The urgency in doing this is to obviously create the best opportunity for patients to recover their eyesight, while also helping to stop the development of other autoimmune diseases, including cancer.
Please realize that the same endocrine immune imbalance that causes SARDS, will also cause autoimmunity and cancer. Unfortunately, untreated SARD patients are waiting for catastrophic diseases to occur!
The following includes clinical data regarding SARDS patients, for your consideration. All of these SARDS patients had ERG’s performed by veterinary ophthalmologists, and all the ERG’s were flat line.
All of these SARDS patients, also had the endocrine immune test performed on them, and with proper hormone therapy, they all regained vision.
The following list contains what I have considered to be clinical comparative, and NOT empirical, endocrine immune levels. The fact that the hormone is present, is no indication that it can be used by the body without measuring the other effects it creates in the body.
NOTE: Salivary tests and 24 hour urine tests provide valuable information on the amount of free hormone that is available for the patient, but they do not indicate whether these free hormones can be used by the body.
The following data and chart will provide you with comparative hormone antibody levels for each SARDS case. The comparison, between normal levels and abnormal levels in these SARDS patients, will be evident.
The normal levels are as follows:
- Total estrogen in a male = 20 to 25 pg/ml
- Total estrogen in a female (spayed and not in heat) = 30 to 35 pg/ml
- Cortisol = 1 to 2.5 ug/dL
- T3 (Triiodothyronine) = 100 to 200 ng/dL (which is active thyroid hormone)
- T4 (Thyroxin) = 2.0 to 4.5 ng/dL (which is a storage thyroid)
- Immunoglobulin A (IgA) = 70 to 170 mg/dL
- Immunoglobulin M (IgM) = 100 to 200 mg/dL
- Immunoglobulin G (IgG) = 1000 to 2000 mg/dL
NOTE: A SARDS blood test result may indicate deficient, normal or elevated cortisol.
If the cortisol is measured, and an elevated total estrogen level is present, it means the normal or elevated cortisol levels are defective and are not active and recognized in the negative feedback mechanism to the hypothalamus and pituitary gland. In this instance, an active cortisol will be used to fund the negative feedback mechanism in order to reduce the elevated adrenal estrogen.
When the cortisol production in a patient is elevated and defective, it should be referred to as an Atypical Cortisol Estrogen Imbalance Syndrome (ACEIS) and not an Atypical Cushing Syndrome. NOTE: Dr. Edward Cushing at the end of the 1930’s reported on 5 or 6 human patients that had pituitary tumors that produced excess amounts of pituitary hormone referred to as ACTH, which caused the middle layer adrenal cortex to produce elevated amounts of active cortisol.
The ACEIS protocol has nothing to do with excessive amounts of active cortisol (Atypical Cushing Syndrome), and only refers to the production of normal and excessive amounts of defective cortisol, and has been inappropriately named by the medical profession.
Along with the fear of using a cortisol supplement, goes the lack of understanding that both you and your canine pet produce 30 to 35 ug/dL of active cortisol from the middle layer adrenal cortex, every day of your lives, in order to remain normal and avoid allergies, autoimmunity and cancer.
If an active cortisol is going to be prescribed for a canine or human for an extended period of time, a thyroid supplement must also be prescribed in order to increase the metabolism of the liver and kidneys, so the active cortisol supplement can be broken down in 24 hours and does not turn into an overdose.
When the total estrogen is elevated, it will bind the receptor sites for T3 and T4, which indicates, even if the T3 and T4 are normal, an active T4 supplement is indicated.
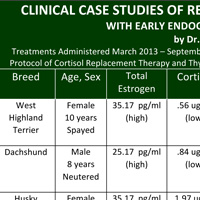
For your consideration, you will find 10 clinical case studies listed below, where blind SARDS dogs have had their vision restored. Below the 10 case studies, there is also a chart which includes the same information.
CASE 1 involved a 10 years old, spayed female, West Highland Terrier.
Her beginning EI panel indicated the following:
- Total estrogen = 35.17 pg/ml which is elevated.
- Cortisol = .56 ug/dL which is deficient.
- T3 = 89 ng/dL which is deficient.
- T4 = .92 ng/dL which is deficient.
- IgA =52 mg/dL which is deficient and too low to absorb oral, replacement cortisol.
NOTE: If the IGA level is below 58, a series of long acting cortisol injections will be indicated at a 10 day interval, to reduce the estrogenic control of the B lymphocyte’s production of IgA, so that an increase in the IgA level will occur up to 58 or higher, and will allow for an oral cortisol replacement, to be absorbed from the intestinal tract.
Once the oral supplementation for this imbalance is completed, the vision does return in many SARDS patients, but only if the SARDS is identified and treated early.
NOTE: For the sake of discussion, all of these patients were also low in the immunoglobulins IgM and IgG.
When the B lymphocyte’s production of immunoglobulins in a canine is suppressed, the IgA, IgM and IgG will all be suppressed, while humans have subpopulations of B lymphocytes that can vary in the amounts of immunoglobulins they may produce.
The importance of these blood test results, once you understand them, will show you the similarity in the endocrine immune imbalances in all SARDS patients. If this imbalance can be identified and corrected early in its development, vision will return to the SARDS patient!
This same imbalance is present in patients with allergies, autoimmune diseases and cancer, even though this imbalance is not recognized by the medical community yet!
Her full vision returned.
CASE 2 involved an 8 year old, male, neutered Dachshund.
His beginning EI panel indicated the following:
- Total estrogen = 25.17 pg/ml. High
- Cortisol = .84 ug/dL. Low
- T3 = 57.6 ng/dL. Low
- T4 =.63 ng/dL. Low
- IgA = 52 mg/dL. Low
His sight returned, once his endocrine immune imbalance was treated, and stopped any further retinal damage.
CASE 3 involved a 7 year old, spayed female, Husky.
Her EI Panel indicated the following:
- Total estrogen = 35.17 pg/ml. High
- Cortisol = 1.97 ug/dL. Normal, but defective
- T3 = 86.24 ng/dL. Low
- T4 = 1.66 ng/dL. Low
- IgA = 57 mg/dL. Low
Her vision has returned, and her far vison is excellent and slightly better than her near vision.
CASE 4 involved a 7 year old, intact, female American Dingo.
Her EI Panel indicated the following:
- Total estrogen = 35.17 pg/ml. High
- Cortisol = 3.10 ug/dL High and defective
- NOTE: Sometimes these defective cortisol levels, can occur as high as 10 and 12 ug/dL or even higher. This is due to the estrogenic block of the thyroid receptor sites and the possibility of a deficient T3 and or T4, which causes the liver and kidney metabolism to be reduced. When this occurs, the breakdown and excretion of the defective cortisol will also be reduced, and a buildup of the elevated, defective cortisol will occur.
- T3 = 64.5 ng/dL. Low
- T4 = .82 ng/dL. Low
- IgA = 53 mg/dL. Low
Her total vision returned in 6 weeks!
CASE 5 involved an 8 year old, spayed female, Maltese.
Her EI Panel indicated the following:
- Total estrogen = 35.20 pg/ml. High
- Cortisol = .44 ug/dL. Low
- T3 = 114.38 ng/dL. Normal, but with estrogenic binding of the thyroid receptor site
- T4 = 2.54 ng/dL. Normal, but with estrogenic binding of the thyroid receptor site
- IgA = 50 mg/dL. Low
It took 3 months for her vision to return.
CASE 6 involved a 5 year old, spayed female, Golden Retriever.
Her EI Panel indicated the following:
- Total estrogen = 35.23 pg/ml. High
- Cortisol = 1.63 ug/ dL. Normal, but defective.
- T3 = 115.23 ng/dL Normal, but with estrogenic binding of the thyroid receptor site
- T4 = 2.20 ng/dL. Normal, but with estrogenic binding of the thyroid receptor site
- IgA = 53 mg/dL. Low
Her vision returned 2 months after her replacement hormone therapy began.
CASE 7 involved a 5 year old spayed, Yorkshire, Terrier mix.
Her EI Panel indicated the following:
- Total estrogen = 35.17 pg/ml. High
- Cortisol = 2.86 ug/dL. High and defective
- T3 = 78.59 ng/dL. Low
- T4 = 1.16 ng/dL. Low
- IgA = 53 mg/dL. Low
Her overall health and allergies are much improved in a short period of time, including far vision. The near vision is expected to happen momentarily.
CASE 8 involved an 8 year old, neutered male, Jack Russell Terrier.
His EI Panel indicated the following:
- Total estrogen = 25.15 pg/ml. High
- Cortisol = 3.54 ug/dL. Hugh and defective
- T3 = 61.23 ng/dL. Low
- T4 = 1.68 ng/dL. Low
- IgA = 51mg/dL. Low
This patient was treated by another veterinarian and sight returned in 3 months.
CASE 9 involved a 7 year old, neutered male, Brussel Griffon.
His EI Panel indicates the following:
- Total estrogen = 25.11 pg/ml. High
- Cortisol = .67ug/dL. Low
- T3 = 124 ng/dL. Normal but with estrogenic binding
- T4 = 3.29 ng/dL. Normal but with estrogenic binding
- IgA = 59 ml/dL. Low
His eye sight has totally returned, however when he eats a food or snack he is allergic too, his vision becomes temporarily reduced and his intestines become inflamed. The reason this happens is because of his IgA, he has developed food sensitivities, and IgA is the mucous membrane antibody that occurs throughout the body, and is in the intestines and in his eyes! Hopefully, this says be very careful with food and snacks you feed your SARDS patient.
CASE 10 involved a 10 year old spayed female, Jack Russell, Pug mix.
Her EI Panel indicated the following:
- Total estrogen = 35.19 pg/ml. High
- Cortisol = 3.47 ug/dL High and defective
- T3 = 63.31 ug/dL. Low
- T4 = 7.2 ug/dL. Low
- IgA = 51 mg/dL
The sight returned to this patient within 4 weeks.

For more complete SARDS analysis, including final EI test results and amounts of replacement hormones used to regain vision on four SARDS case studies, please read SARDS Clinical Case Studies.
GENERAL THOUGHTS ABOUT SARDS
SARDS is a multisystem disorder that is caused by an endocrine immune imbalance.
Uncorrected blindness may be the least of the health problems a SARDS patient faces, due to their endocrine immune imbalance!
In order for vision to return to a SARDS patient, immediate testing and endocrine immune correction is required.
Only waiting to see what is going to happen with your SARDS patient, will happen!
Please be aware of the fact that food allergies, foods containing phytoestrogens, trypsin deficiencies, chemicals, and malabsorption, may play a big role in determining whether the replacement hormones you are giving your SARDS patient will be effective or not.
The longer you wait to act, the better the chances your SARDS patient will be permanently blind.
Even if your pet has had SARDS for 6 months or longer, it is still worth trying to regain far vision. But what is even more important than the far vision, is helping to stop the development of other autoimmune diseases and cancer.
Where there is life, there will always be hope, and when a treatment for a disease has not yet been discovered or accepted, a treatment can still exist.
These are only my thoughts, and I hope they will give you hope for your SARDS pet and help make a difference.
By looking at the various SARDS Journeys on this website, you can actually view some of these blinds dogs that have had their SARDS endocrine immune imbalance corrected, and see them with their sight returned on their owner’s videos! (Emmi’s Adventure with SARDS, Lexie’s Journey With SARDS, Shasta’s Battle With SARDS)
Sincerely,
Dr. AL Plechner